Trusted by Law Enforcement & Tactical Professionals
Roadside Trauma: What to Carry Before EMS Arrives
7 min reading time
Arterial bleeding kills in 3–5 minutes. EMS averages 14 minutes nationally. Stage the right gear in your vehicle cabin — and know the MARCH sequence — before you need it.
The national average EMS response time is 14 minutes. In rural counties it runs past 30. In the time between a crash and the ambulance arriving, uncontrolled bleeding from a single arterial wound can kill a person in three to five minutes. The gear staged in your vehicle determines whether those minutes cost a life.
The Federal Highway Administration records more than six million crashes annually in the United States. A fraction involve severe trauma — but when they do, the first person with capable hands and the right gear is almost always a civilian. That might be a bystander. It might be you. This guide covers what to carry, where to stage it, and how to execute the MARCH framework at a crash scene when the ambulance is still 14 minutes out.
What You Are Actually Responding To
Vehicle crashes produce a predictable injury pattern. Knowing it before you arrive at a scene shapes what gear matters most.
Extremity hemorrhage — door intrusion, broken glass, and seatbelt cut injuries produce lacerations and punctures. The mechanism is fast and the arterial risk is real.
Thoracic trauma — steering column and airbag impacts can produce rib fractures, pulmonary contusion, and in penetrating crashes, pneumothorax risk.
Head and airway compromise — high-energy impacts produce concussion and unconsciousness. A casualty who cannot protect their own airway needs help immediately.
Hypothermia and shock — crash victims lose core temperature rapidly. Hemorrhagic shock accelerates that loss. A Mylar blanket is not optional.
MARCH at the Scene: Work the Sequence
MARCH — Massive Hemorrhage, Airway, Respiration, Circulation, Hypothermia — is the treatment sequence every U.S. military branch and most law enforcement agencies use to work through trauma priorities. Apply it in order. Do not skip ahead.
M — Massive Hemorrhage
Identify any limb bleeding first. Arterial bleed — bright red, spurting, pressure-cycling with the heartbeat — requires a CAT Gen 7 or SOFTT-W tourniquet applied two inches above the wound. Tighten until the bleeding stops. Write the application time on the casualty's forehead with a marker. For junctional or truncal bleeds a tourniquet cannot reach, pack the wound with QuikClot Combat Gauze and hold direct pressure for three full minutes without lifting.
A — Airway
If the casualty is unconscious, check for airway obstruction. Use a jaw-thrust — not head-tilt/chin-lift, which risks the cervical spine — to open the airway. A 28 French NPA with water-based lubricant manages an unresponsive casualty's airway until EMS arrives.
R — Respiration
Look for asymmetrical chest rise, penetrating thoracic trauma, or a sucking chest wound. Apply vented chest seals to both entry and exit wounds. The vented design allows trapped air to escape and prevents tension pneumothorax. A casualty breathing shallow and fast with declining consciousness needs this before anything else in this step.
C — Circulation / H — Hypothermia
Reinforce any wound packing or dressings. Apply a Mylar emergency blanket. Crash victims lose core temperature rapidly — hypothermia accelerates coagulopathy and compounds hemorrhage. Wrap them and keep them wrapped until EMS arrives.
Field Note: Write the Time
Write the tourniquet application time on the casualty's forehead or forearm with a permanent marker — not on the tourniquet tab where it can smear. EMS and the ER team need that timestamp to manage limb viability. More than 4,000 documented combat applications since 2005 confirm tourniquet use saves lives. Do not delay application out of hesitation. An unnecessary tourniquet is reversible. An uncontrolled arterial bleed is not.
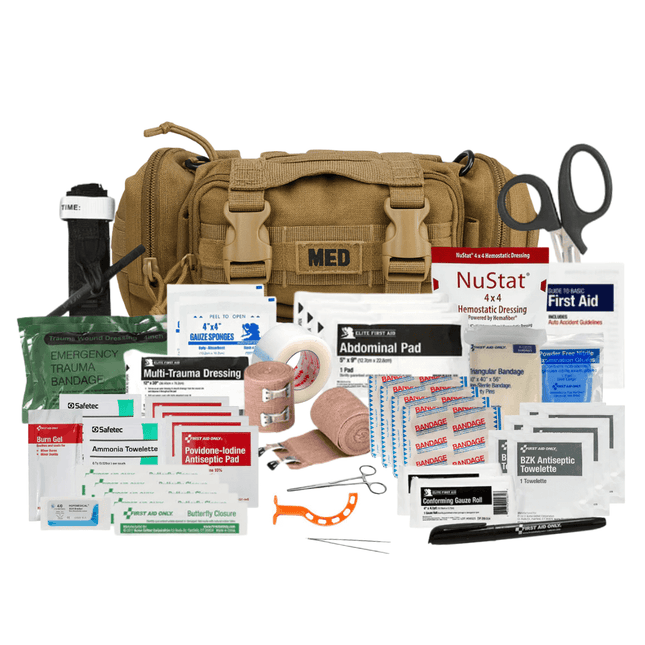
What to Carry in the Vehicle
A household first aid kit does not close the gap between a crash and an ambulance. These are the components that do.
The trunk is the wrong answer for primary trauma gear. In a rear-end collision the trunk may be inaccessible or compromised. The driver needs to reach bleeding control in the first 60 seconds, often from a seated position with one usable hand.
Under the driver's seat — accessible from seated position, protected from UV, stays dry.
Center console — ideal for compact kits in smaller vehicles. Grab-and-go from driver or passenger.
Seat-back MOLLE or rip-away pouch — passenger-accessible, visible on approach from outside the vehicle.
Trunk: secondary kit only — larger capacity for extended travel or multi-casualty, not the primary bleed-control platform.
Am I legally protected if I use my kit on someone else at a crash scene?
Good Samaritan laws protect civilians who render emergency care in good faith in all 50 U.S. states. No medical license is required for the gear or for using it. They do require acting within your training level. The legal exposure of doing nothing while someone bleeds out is greater than the legal exposure of applying a tourniquet correctly.
Should I move the casualty out of the vehicle?
Move only if the vehicle presents immediate danger — fire, submersion, or active structural collapse. For hemorrhage control you do not need the casualty out of the vehicle. Reach in, expose the wound, apply the tourniquet or dressing in place. EMS is trained for extraction. Your job is to keep them alive until EMS arrives.
How do I know if the bleeding requires a tourniquet?
Arterial bleeding is bright red and pulses with the heartbeat — it spurts rather than seeps. Both arterial and venous bleeding from major wounds require immediate pressure. Arterial bleeding on an extremity requires a tourniquet. If you cannot tell the difference under stress, apply the tourniquet. An unnecessary tourniquet is safer than an uncontrolled arterial bleed.
Bottom Line
The crash ends in seconds. The survivable injury window is three to five minutes. What you carry in the cabin — staged correctly, inspected annually — is the difference between applying pressure until EMS arrives and watching someone bleed out while waiting. A household first aid kit does not close that gap.
If you have not taken a Stop the Bleed class, stopthebleed.org offers free two-hour certification in every state.
In Stock
Domestic Shipping (USA - Lower 48 Only) Orders are processed within 24 hours and typically ship within 1–2 business days. Once shipped, delivery takes an estimated 3–7 days, with most orders arriving in just 5 days. Please Note: We currently do not ship to Alaska, Hawaii, or international destinations. Questions? Contact us anytime at support@vitacsolutions.com or call 307-202-8426.
In Stock
Domestic Shipping (USA - Lower 48 Only) Orders are processed within 24 hours and typically ship within 1–2 business days. Once shipped, delivery takes an estimated 3–7 days, with most orders arriving in just 5 days. Please Note: We currently do not ship to Alaska, Hawaii, or international destinations. Questions? Contact us anytime at support@vitacsolutions.com or call 307-202-8426.
In Stock
Domestic Shipping (USA - Lower 48 Only) Orders are processed within 24 hours and typically ship within 1–2 business days. Once shipped, delivery takes an estimated 3–7 days, with most orders arriving in just 5 days. Please Note: We currently do not ship to Alaska, Hawaii, or international destinations. Questions? Contact us anytime at support@vitacsolutions.com or call 307-202-8426.
In Stock
Domestic Shipping (USA - Lower 48 Only) Orders are processed within 24 hours and typically ship within 1–2 business days. Once shipped, delivery takes an estimated 3–7 days, with most orders arriving in just 5 days. Please Note: We currently do not ship to Alaska, Hawaii, or international destinations. Questions? Contact us anytime at support@vitacsolutions.com or call 307-202-8426.
What are you preparing for? On-duty response, family preparedness, outdoor adventure... Answer 5 quick questions and we'll match you with the right gear.
Cold environments demand deliberate gear decisions. This guide covers the three-layer system — base, mid, and shell — from a preparedness standpoint: how each layer...
Identify Fake Gear: Ensuring Your Trauma Kits Meet TCCC Standards
Counterfeit CAT tourniquets fail under pressure. TCCC-standard gear has specific markings, materials, and testing — here's how to verify before your kit is tested for...
Uncontrolled bleeding is the leading cause of preventable trauma death. EMS averages 14 minutes nationally. A firearm stops the threat — only a trauma kit...
We've been downrange. We know what it costs to be unprepared. ViTAC was built by U.S. Army Special Operations veterans to make sure the people who run toward the threat — and the families who depend on them — have gear that works when everything is on the line.
— ViTAC Solutions Founders | 40+ years combined Special Operations experience
Most of our trauma kits and first aid supplies qualify for HSA and FSA reimbursement. Don't let your benefits expire — invest them in gear that could save a life.
The item was as promised. Everything in the kit was high-quality and I’m pleased with that. The only problem I have is I’m not sure it’s worth the cost. I found all of the contents individually for significantly less money. The only thing I didn’t find on my own was the pouch everything came in and that was a perfect fit so I would give it an A plus on quality, but a C on value.