Preparing for Field Injuries When Help Is 30 Minutes Away
7 min reading time
First aid for remote injuries is crucial when help is delayed. This guide outlines essential steps and items to prepare for emergencies in the backcountry.
The average EMS response time in rural areas of the United States exceeds 18 minutes. In genuinely remote terrain, that figure extends well beyond 30 to 60 minutes or more. During that interval, the decisions and actions taken by whoever is on scene determine whether an injured person survives with minimal complications or deteriorates into a preventable death.
This guide covers what to carry, what to do first, how to manage an injured person while waiting for evacuation, and how to verify your kit is ready before you leave the trailhead.
Primary Assessment: MARCH Before Anything Else
TCCC and Wilderness EMS both sequence field trauma response using the MARCH protocol. Work through it in order — do not advance to the next step until you have addressed the current one:
Priority
Assessment Focus
Field Action
M — Massive Hemorrhage
Is the patient bleeding at a life-threatening rate?
Tourniquet for limb bleeds; wound pack with hemostatic gauze for junctional wounds
A — Airway
Is the airway open and clear?
Head-tilt/chin-lift or NPA if unconscious; recovery position if breathing
R — Respiration
Is the patient breathing adequately?
Seal sucking chest wounds with vented chest seals; begin rescue breathing if no pulse
C — Circulation
Are secondary bleeds controlled? Is shock developing?
Direct pressure on secondary wounds; lay flat, elevate legs if no spinal injury suspected
H — Hypothermia
Is the patient at risk for heat loss?
Wrap in Mylar or thermal blanket; remove wet clothing; shield from wind
Field Note: Scene Safety Is the First Intervention
Scene safety comes before patient contact. If the hazard that injured the first person can injure you — unstable terrain, active traffic, downed electrical lines — your role is to call for help and wait. Do not become a second casualty.
Managing the Patient While Awaiting Evacuation
Hemorrhage — Active and Secondary
Apply a tourniquet high and tight on any limb with arterial bleeding — do not hesitate. Write the time on the tourniquet or the patient's skin immediately. For torso, neck, or groin wounds where a tourniquet cannot be placed, pack the wound firmly with hemostatic gauze and apply sustained manual pressure for a minimum of three minutes. Add material on top of blood-soaked dressings without removing the original layer.
Fractures and Sprains
Immobilize in the position found unless distal circulation is absent. Splint above and below the injury using a SAM splint, improvised materials, or a wrapped and padded limb. Pad all bony prominences to prevent pressure sores during extended evacuation holds. For sprains, wrap with an elastic bandage and confirm capillary refill in fingers or toes — if refill time exceeds 2 seconds, the bandage is too tight.
Shock Prevention
Hypovolemic shock follows uncontrolled bleeding and presents as pale or grey skin, rapid weak pulse, confusion, and cold extremities. Keep the patient supine; elevate the legs 12 inches if no spinal or lower-extremity fracture is suspected. Prevent heat loss aggressively — shock and hypothermia are mutually reinforcing. Do not offer fluids to a potentially surgical patient or anyone with altered level of consciousness.
Ongoing Patient Monitoring
Reassess every 15 minutes for serious injuries, every 30 minutes for stable patients. Track and record:
Level of consciousness (AVPU: Alert, Voice, Pain, Unresponsive)
Respiratory rate and quality
Pulse rate and strength
Skin color and temperature
Pain level (0–10 scale)
Tourniquet application time (if applicable)
Fluid input and any output (urine, vomit, blood loss)
This record transfers directly to the receiving EMS or trauma team. If you have satellite communication capability, relay vitals with your position and mechanism of injury.
Kit Organization for Rapid Access
Organize by treatment priority, not by body system. Under stress, your hand should reach the right item first:
Compartment / Layer
Contents
Outermost / Top
Tourniquet, chest seals, nitrile gloves — life-threat items only
Sterile gauze pads, medical tape, antiseptic wipes, SAM splint, elastic bandages
Main — Rear
Medications, instant cold packs, Mylar blanket, CPR mask, personal prescriptions
Outer Pocket
Emergency contacts, medical history sheet, permanent marker
Group items within each layer using labeled clear zip bags. A kit you can navigate in 10 seconds in daylight should take no longer than 20 seconds in the dark. Practice it.
Pre-Trip Readiness Check
Run this before every trip — not once a season:
Expiration dates: Check all medications, ointments, and sterile supplies. Expired sterile packaging is not sterile.
Packaging integrity: Torn wrappers, leaking seals, dried antiseptic wipes — replace all.
Quantity audit: Verify you have enough high-use items (bandages, gauze, gloves) for your group size and trip duration.
Functionality: Trauma shears should cut cleanly; closures and zippers should operate without friction.
Personal prescriptions: EpiPens, inhalers, cardiac medications — confirm they are present and current.
Field Note: A Pre-Trip Inventory Takes Five Minutes
A kit with missing or expired components is not a functional kit. Running a pre-trip inventory takes five minutes. Discovering the gap during an emergency is not recoverable.
ViTAC Kits for Remote Field Use
Purpose-built kits reduce the margin for missed components and eliminate the risk of substandard substitutions. For the decision matrix on kit type by trip profile, see Camping First Aid Kit vs. Trauma Kit: Which Do You Need?
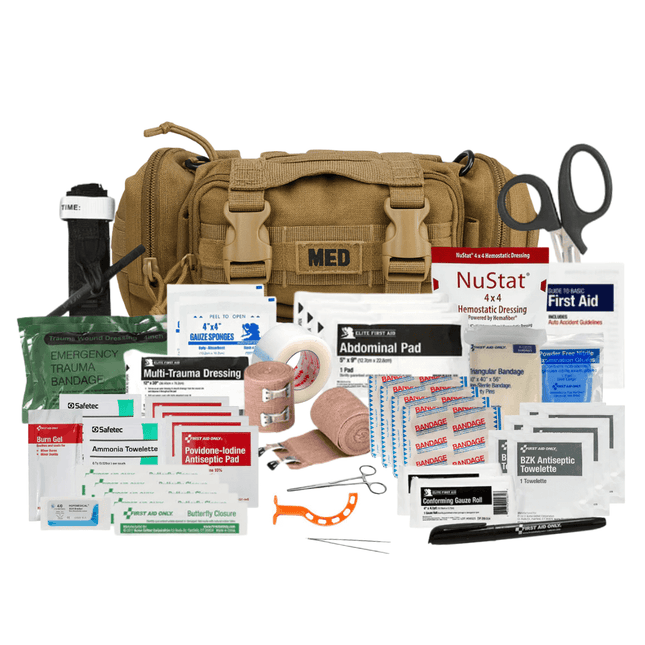
Rip-Away Tactical Trauma Kit — MOLLE-compatible fast-deploy kit with MARCH-sequenced components; built for pack or belt carry in field conditions
What are the most important items in a remote field first aid kit?
MARCH priorities drive the answer. A TCCC-approved tourniquet, hemostatic gauze, and pressure bandage cover massive hemorrhage. Vented chest seals address penetrating chest wounds. A Mylar blanket, nitrile gloves, and irrigation syringe complete the primary tier. General wound care supplies build from there.
What do I do first when someone is seriously injured far from help?
Confirm scene safety, then work MARCH: Massive hemorrhage first (tourniquet or wound pack), Airway, Respiration, Circulation, Hypothermia. Do not advance to the next priority until the current one is addressed. Record tourniquet application time immediately.
How often should I check and restock my kit?
Before every trip. Replace what was used, verify expiration dates, confirm packaging integrity. Do not assume the kit is ready because it was packed before the last trip.
Bottom Line
When help is 30 minutes out, the outcome is largely determined in the first five minutes. MARCH gives you the sequence. A pre-built, organized, verified kit gives you the tools. Training gives you the execution under stress.
In Stock
Domestic Shipping (USA - Lower 48 Only) Orders are processed within 24 hours and typically ship within 1–2 business days. Once shipped, delivery takes an estimated 3–7 days, with most orders arriving in just 5 days. Please Note: We currently do not ship to Alaska, Hawaii, or international destinations. Questions? Contact us anytime at support@vitacsolutions.com or call 307-202-8426.
In Stock
Domestic Shipping (USA - Lower 48 Only) Orders are processed within 24 hours and typically ship within 1–2 business days. Once shipped, delivery takes an estimated 3–7 days, with most orders arriving in just 5 days. Please Note: We currently do not ship to Alaska, Hawaii, or international destinations. Questions? Contact us anytime at support@vitacsolutions.com or call 307-202-8426.
In Stock
Domestic Shipping (USA - Lower 48 Only) Orders are processed within 24 hours and typically ship within 1–2 business days. Once shipped, delivery takes an estimated 3–7 days, with most orders arriving in just 5 days. Please Note: We currently do not ship to Alaska, Hawaii, or international destinations. Questions? Contact us anytime at support@vitacsolutions.com or call 307-202-8426.
In Stock
Domestic Shipping (USA - Lower 48 Only) Orders are processed within 24 hours and typically ship within 1–2 business days. Once shipped, delivery takes an estimated 3–7 days, with most orders arriving in just 5 days. Please Note: We currently do not ship to Alaska, Hawaii, or international destinations. Questions? Contact us anytime at support@vitacsolutions.com or call 307-202-8426.
What are you preparing for? On-duty response, family preparedness, outdoor adventure... Answer 5 quick questions and we'll match you with the right gear.
We've been downrange. We know what it costs to be unprepared. ViTAC was built by U.S. Army Special Operations veterans to make sure the people who run toward the threat — and the families who depend on them — have gear that works when everything is on the line.
— ViTAC Solutions Founders | 40+ years combined Special Operations experience
Most of our trauma kits and first aid supplies qualify for HSA and FSA reimbursement. Don't let your benefits expire — invest them in gear that could save a life.
Good quality products. The free items were also nice. Great med kit for alot of travel situations
Thank you for the 5-star review. We’re glad the med kit and added items delivered value and that it’s serving you well for travel. Stay prepared and safe out there.
The item was as promised. Everything in the kit was high-quality and I’m pleased with that. The only problem I have is I’m not sure it’s worth the cost. I found all of the contents individually for significantly less money. The only thing I didn’t find on my own was the pouch everything came in and that was a perfect fit so I would give it an A plus on quality, but a C on value.
Thank you for the honest feedback. We’re glad the kit quality and pouch met the mark. We understand your point on value, our pricing reflects not only the components, but careful sourcing, organization, and readiness in one dependable setup. We appreciate your support.